Overview
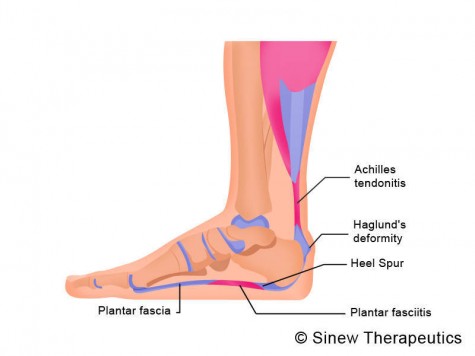
Pain at the posterior heel or posterior ankle is most commonly caused by pathology at the posterior calcaneus, the Achilles (calcaneal) tendon, or the associated bursae. The following bursae are located just superior to the insertion of the Achilles tendon. Subtendinous calcaneal bursa. This bursa (also called the retrocalcaneal bursa), situated anterior (deep) to the Achilles tendon, is located between the Achilles tendon and the calcaneus. Subcutaneous calcaneal bursa. Also called the Achilles bursa, it is found posterior (superficial) to the Achilles tendon, lying between the skin and the posterior aspect of the distal Achilles tendon. Inflammation of one or both of these bursae can cause pain in the posterior heel and ankle regions.
Causes
The most common causes of bursitis are injury or overuse, although infection may also be a cause. Bursitis is also associated with other causes, such as arthritis, gout, tendinitis, diabetes, and thyroid disease.
Symptoms
Pain and tenderness are common symptoms. If the affected joint is close to the skin, as with the shoulder, knee, elbow, or Achilles tendon, swelling and redness are seen and the area may feel warm to the touch. The bursae around the hip joint are deeper, and swelling is not obvious. Movement may be limited and is painful. In the shoulder, it may be difficult to raise the arm out from the side of the body. Putting on a jacket or combing the hair becomes a troublesome activity. In acute bursitis symptoms appear suddenly, with chronic bursitis, pain, tenderness, and limited movement reappear after exercise or strain.
Diagnosis
Careful examination by your physician or physiotherapist can determine if the inflammation is from the Achilles tendon or from the retrocalcaneal bursa. Tenderness due to insertional Achilles tendinitis is normally located slightly more distal where the tendon inserts into the back of the heel, whereas tenderness caused by the retrocalcaneal bursa is normally palpable at the sides of the distal Achilles tendon. Diagnosis can be confirmed with an ultrasound investigation, MRI or CT scan.
Non Surgical Treatment
The initial treatment for retrocalcaneal bursitis is to avoid activities that cause pain and take non-steroidal anti-inflammatory medications (for example, ibruprofen). Your doctor may recommend icing the heel several times a day and may prescribe physical therapy to improve flexibility and strength around the ankle. Physical therapy serves two functions, it can help the bursitis improve and it can help prevent future recurrences.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
 Overview
Overview Symptoms
Symptoms Overview
Overview Symptoms
SymptomsMBO44QsjS,!~~60_35.JPG)





 Achilles tendonitis is an iInflammation in the tendon of the calf muscle, where it attaches to the heel bone. Achilles tendonitis causes pain and stiffness at the back of the leg, near the heel. Achilles tendonitis can be caused by overuse of the Achilles tendon, overly tight calf muscles or Achilles tendons, excess uphill running, a sudden increase in the intensity of training or the type of shoes worn to run, or wearing high heels at work and then switching to a lower-heeled workout shoe. Achilles tendonitis causes pain, tenderness, and often swelling over the Achilles tendon. There is pain on rising up on the toes and pain with stretching of the tendon. The range of motion of the ankle may be limited. Treatment includes applying ice packs to the Achilles tendon, raising the lower leg, and taking an anti-inflammatory medication. In some severe cases of Achilles tendonitis, a cast may be needed for several weeks. A heel lift insert may also be used in shoes to prevent future overstretching of the Achilles tendon. Exerting rapid stress on the Achilles tendon when it is inflamed can result in rupture of the tendon.
Achilles tendonitis is an iInflammation in the tendon of the calf muscle, where it attaches to the heel bone. Achilles tendonitis causes pain and stiffness at the back of the leg, near the heel. Achilles tendonitis can be caused by overuse of the Achilles tendon, overly tight calf muscles or Achilles tendons, excess uphill running, a sudden increase in the intensity of training or the type of shoes worn to run, or wearing high heels at work and then switching to a lower-heeled workout shoe. Achilles tendonitis causes pain, tenderness, and often swelling over the Achilles tendon. There is pain on rising up on the toes and pain with stretching of the tendon. The range of motion of the ankle may be limited. Treatment includes applying ice packs to the Achilles tendon, raising the lower leg, and taking an anti-inflammatory medication. In some severe cases of Achilles tendonitis, a cast may be needed for several weeks. A heel lift insert may also be used in shoes to prevent future overstretching of the Achilles tendon. Exerting rapid stress on the Achilles tendon when it is inflamed can result in rupture of the tendon.




You must be logged in to post a comment.